Aspect | Internal Hemorrhoids | External Hemorrhoids |
Pathophysiology | Swollen/inflamed vascular structures in the anal canal. | It is the same as internal but can be externally visible. |
"Sliding theory": Downward displacement of anal cushions due to weakened connective tissues. | Increased venous pressure and swelling in the inferior hemorrhoidal veins, rather than the downward displacement of anal cushions seen in internal hemorrhoids. | |
Signs & Symptoms | - Grade 1: Bleeds, no prolapse. | Typically painful if thrombosed. |
- Grade 2: Prolapse during bowel movements, reduces spontaneously. | It may cause swelling and irritation. | |
- Grade 3: Requires manual reduction. | ||
- Grade 4: Cannot be reduced. | ||
Conservative Management | High-fiber diet, increased fluids, stool softeners, hydrocortisone suppositories. | Warm sitz baths, topical creams. |
Specific Treatments | - Grade 1 & 2: Sclerotherapy, Rubber band ligation. | Thrombosed Hemorrhoids: |
- Grade 3 &4: Hemorrhoidectomy, Stapled hemorrhoidopexy. | - Within 72 hours: Excision. | |
- After 72 hours: Conservative management. |
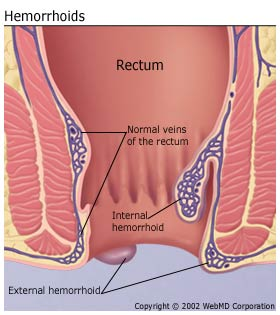
Image source: Padmavathi Gastroenterology Clinic. Available at: padmavathigastro.com
Pathophysiology of Hemorrhoids
Hemorrhoids, commonly referred to as piles, are vascular structures in the anal canal that help with stool control. They become an issue when swollen or inflamed, classified as hemorrhoidal disease. The "sliding theory" suggests that hemorrhoids develop when the anchoring connective tissues of the anal cushions deteriorate. This leads to the downward displacement of the anal cushions, which disrupts the vascular flow, causing venous dilation and the formation of hemorrhoids.
Signs and Symptoms
Internal Hemorrhoids:
Grade 1: May bleed but do not prolapse.
Grade 2: Prolapse during bowel movements but reduces spontaneously.
Grade 3: Prolapse during bowel movements and requires manual reduction.
Grade 4: Prolapse and cannot be manually reduced.
External Hemorrhoids:
Typically painful if thrombosed.
It may cause swelling and irritation around the anus.
Management of Hemorrhoids
Internal Hemorrhoids:
Conservative Treatment: Includes high-fiber diets, increased fluid intake, stool softeners, and topical treatments (e.g., suppositories containing hydrocortisone).
Grade 1 & 2 Treatments:
Sclerotherapy: In Grade 1, only Injection of a solution that causes the hemorrhoid to shrink.
Rubber Band Ligation: Placement of a tight band around the base of the hemorrhoid to cut off blood supply, causing it to fall off.
Grade 3 & 4 Treatments:
Hemorrhoidectomy: Surgical removal of excessive tissue causing bleeding and prolapse.
Stapled Hemorrhoidopexy: Re-sectioning of the prolapsed hemorrhoidal tissue and repositioning back to the original anatomical position.
External Hemorrhoids:
Conservative Treatment: Includes warm sitz baths and topical creams to ease symptoms.
Thrombosed External Hemorrhoids:
If presented within 72 hours, excision under local anesthesia can be considered to relieve pain rapidly.
After 72 hours, conservative management is recommended as the body gradually reabsorbs the clotted blood.
Comments